Address
30 N Gould St.
Suite R, Sheridan, WY 82801, USA
Ipamorelin vs Semaglutide: Key Differences in Fat Loss and Body Composition
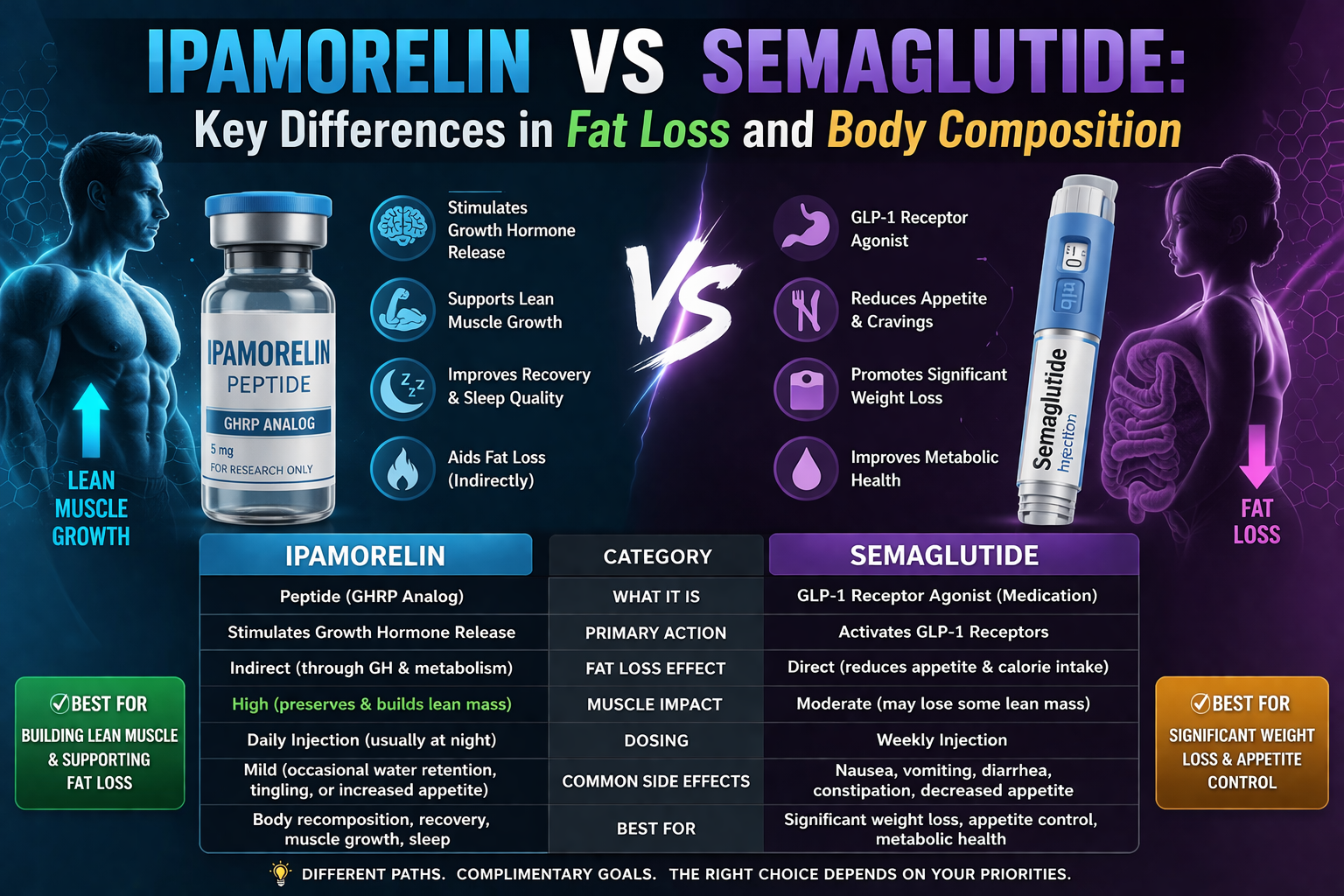
So, which one actually helps you change your fat and body shape more: a growth-hormone secretagogue like ipamorelin or a GLP-1 drug like semaglutide? Semaglutide tends to deliver bigger, more reliable weight loss and appetite control, while ipamorelin is better for holding onto or improving lean mass—especially if you’re training and eating well.
If you mainly want to drop pounds and curb hunger, semaglutide usually works faster and harder. If you’re aiming to keep or build muscle while losing fat, ipamorelin or growth-hormone protocols offer more, especially with resistance workouts.
Key Takeaways
- Pick semaglutide if you want strong, steady weight loss.
- Pick ipamorelin if you want to preserve or build muscle with your training.
- Think about your goals, safety, and what you can actually get before you decide.
Understanding Ipamorelin and Semaglutide
Let’s break down what each drug is, how it works, and why they don’t affect fat loss or body composition in the same way. Here’s a look at their chemical class, typical uses, and what they do to appetite, metabolism, and fat stores.
What Is Ipamorelin?
Ipamorelin is a growth hormone releasing peptide (GHRP). You get it as a short peptide that tells your pituitary to pump out more growth hormone (GH).
Clinicians use it to help with lean mass, recovery, and sometimes low GH from aging. You’ll see low to moderate GH bumps without the big jumps in cortisol or prolactin that older GHRPs can cause.
That usually means modest muscle gains, better sleep, and some extra fat burning over weeks or months. Doctors give it by injection, often daily or at night, and usually pair it with a good diet and exercise plan.
People use ipamorelin to keep muscle during calorie cuts or to speed up recovery. Side effects are usually mild—think injection site soreness, some water retention, or maybe a little more appetite for some folks.
What Is Semaglutide?
Semaglutide is a GLP-1 receptor agonist approved for type 2 diabetes and long-term weight management. It mimics the hormone GLP-1, which slows down your stomach and makes you less hungry.
You take semaglutide as a once-a-week subcutaneous injection. Clinical trials show big weight loss when you combine it with diet and exercise.
You’ll probably notice less hunger, smaller meals, and better blood sugar in a few weeks. Most side effects hit your stomach: nausea, constipation, sometimes vomiting or reflux.
Doctors usually start with low doses and slowly ramp up to limit side effects and keep an eye on your metabolism. Semaglutide attacks calorie intake and blood sugar directly, so it’s generally more powerful for fat loss than peptides that work indirectly.
Mechanisms of Action
Ipamorelin binds to ghrelin receptors in your pituitary and hypothalamus, triggering pulses of GH release. That GH pulse boosts IGF-1, helps you build protein, burn fat, and repair tissue.
How much body fat you lose depends on how active you are, your protein intake, and your overall calories. Semaglutide turns on GLP-1 receptors in your brainstem and gut.
This makes you less hungry, fills you up faster, and slows your digestion, so you eat less overall. It also improves insulin release and drops glucagon, which helps with fat loss by evening out your blood sugar and dialing down fat storage signals.
Key differences in action:
- Ipamorelin: triggers GH → better lean mass, modest fat burning.
- Semaglutide: controls appetite and blood sugar → bigger, faster calorie and weight drops.
Key Differences in Fat Loss Mechanisms
Ipamorelin mainly raises growth hormone, while semaglutide cuts appetite and improves blood sugar. These two routes change your body in different ways—think speed of weight loss, muscle retention, and side effects.
How Ipamorelin Promotes Fat Loss
Ipamorelin is a growth hormone releasing peptide. You inject it to nudge your pituitary to release more GH, which then boosts IGF-1 and breaks down fat over time.
Because GH supports muscle protein synthesis, you’re more likely to keep muscle during a calorie deficit. That means a bigger chunk of your weight loss comes from fat, not muscle.
Results come slow and steady—don’t expect the scale to drop overnight. Some people notice better recovery, more workout energy, and a slight metabolic kick.
Side effects are usually mild: maybe a bit of water retention or achy joints for some. It’s smart to have a doctor check in on you during use.
How Semaglutide Influences Fat Reduction
Semaglutide is a GLP-1 receptor agonist that kills your appetite and slows how fast your stomach empties. You eat less because you’re less hungry and feel fuller, which leads to a calorie deficit and weight loss.
It also makes your body handle insulin better and drops blood sugar, which helps prevent fat from building up—especially around your belly. Semaglutide’s effects are mostly about eating less and better metabolism, not building muscle.
You’ll probably lose more total weight with semaglutide than with ipamorelin alone. Side effects? Mostly nausea, constipation, or mild GI issues, especially at first. Adjusting the dose and regular follow-ups help keep things manageable.
Fat Loss Onset and Duration of Effects
Ipamorelin usually takes weeks or months to show changes. You’ll need daily injections and regular resistance training for the best shot at keeping muscle and losing fat.
Semaglutide often shows visible weight loss in 4–12 weeks as your appetite shrinks. Most people see bigger drops over a few months as long as they stick with the medication and keep calories in check.
But the effects don’t last forever. If you stop ipamorelin, GH benefits fade and fat loss slows. Stop semaglutide, and appetite and weight often creep back unless you stick to your new habits. It’s worth talking to your doctor about long-term plans.
Impact on Body Composition
Ipamorelin and semaglutide both lower body fat, but they do it differently: one protects or builds lean tissue, the other cuts fat mostly by shrinking appetite and calories. They also change muscle, visceral fat, and overall recomposition in their own ways.
Changes in Lean Muscle Mass
Ipamorelin often helps you keep lean mass because it triggers growth hormone. That means more protein synthesis and a better shot at gaining or holding muscle—if you’re lifting and eating enough protein.
Studies and real-world stories show modest muscle gains, especially in older adults who start with low GH. Semaglutide doesn’t raise growth hormone, so weight loss from it can include some muscle loss along with fat loss.
Some research says lean mass loss is small, others say it’s bigger if you lose a lot of weight. If you’re using semaglutide, aim for regular strength training and about 1.2–1.6 g protein per kilo of body weight to help protect muscle.
Effects on Visceral Fat
Semaglutide is pretty reliable for lowering visceral fat since it cuts calories and boosts insulin sensitivity. Trials show solid drops in belly fat and markers linked to metabolic risk.
That’s true even if you lose a bit of muscle—it still improves your health profile. Ipamorelin can cut visceral fat too, but mostly by raising your metabolic rate and building muscle.
The evidence there is smaller and less predictable than with semaglutide. If you want fast, proven visceral fat loss, semaglutide wins; if you want some metabolic perks and muscle support, ipamorelin might help—especially if you’re working out.
Overall Body Recomposition
If you’re chasing fat loss with muscle retention, you’ll want to match the right drug with your training and diet. Ipamorelin plus resistance training usually shifts your body toward more muscle and less fat, though it’s a slower process.
Semaglutide leads to bigger total weight and fat drops for most people since it cuts appetite and calories. But you’ll need to keep up exercise and protein to avoid losing too much muscle.
Some doctors even combine both under supervision to try for strong fat loss and muscle protection—but don’t do that without medical guidance.
Clinical Evidence and Research Comparisons
Ipamorelin research mostly looks at growth hormone release and body composition, while semaglutide trials focus on blood sugar and significant, steady weight loss. The size and quality of research is pretty different between them.
Ipamorelin Clinical Studies
Most ipamorelin studies are small and kind of exploratory. Researchers usually measure hormonal responses: you’ll see repeated tests showing more GH pulses and sometimes IGF-1 after dosing.
Those hormone jumps can link to fat loss and muscle retention, but big, long-term weight loss studies are rare. Most trials last weeks or a few months and only have a handful of participants.
So, we don’t really know much yet about its effects on lasting weight loss or health outcomes. Mechanistic data is there, but outcome trials? Not so much.
Semaglutide Research Outcomes
Semaglutide has big, randomized, placebo-controlled trials with clear weight loss and better blood sugar. Phase 3 obesity studies had thousands of people and showed average weight drops often in the double-digits (percent) over 68 weeks with lifestyle help.
Trials also found better blood sugar, blood pressure, and some heart risk markers in folks with diabetes. Dosing followed a weekly injection schedule, ramped up over time.
Side effects were mostly stomach-related and usually mild or moderate. Long-term studies give us more robust safety and effectiveness data than we have for ipamorelin.
Comparative Effectiveness Data
No one’s really done head-to-head trials between ipamorelin and semaglutide. You have to compare small hormone studies for ipamorelin with big outcome trials for semaglutide.
That makes semaglutide the better evidence-based choice for real, lasting weight loss in clinical settings. If you want proven fat loss and metabolic gains, semaglutide has the best data.
If you’re more interested in GH signaling and maybe tweaking your body composition, ipamorelin shows some promise, but we just don’t have big trials yet. Always weigh safety, your goals, and the strength of the evidence.
Safety Profiles and Side Effects
Ipamorelin mostly boosts growth hormone with few stomach issues, while semaglutide works on appetite and glucose and can cause more digestive and metabolic side effects. Both have their own risks and need some monitoring before you start.
Ipamorelin Safety Overview
Ipamorelin boosts your growth hormone (GH) and IGF-1 by nudging the pituitary into action. You might notice mild water retention, headaches, or numbness where you inject—usually tied to the dose and often fading within days or weeks.
Unlike some other GH secretagogues, ipamorelin doesn’t usually spike cortisol or prolactin, so there’s a bit less endocrine risk. People with active cancer, untreated pituitary tumors, or proliferative diseases should steer clear, since GH/IGF-1 can push tumor growth.
Keep an eye out for joint pain or rare bumps in fasting glucose. Medications that mess with hormones can interact, so tell your provider what you’re taking. Regular checks of IGF-1, fasting glucose, and symptoms help catch issues early.
Semaglutide Risk Factors
Semaglutide acts as a GLP-1 receptor agonist. Most people run into nausea, vomiting, diarrhea, constipation, or just less appetite—these GI side effects usually ease up after a few weeks.
Serious risks like pancreatitis, gallbladder disease, or kidney injury from dehydration are rare but possible if you’re unlucky with vomiting or diarrhea.
If you or your family have a history of medullary thyroid carcinoma or MEN2, semaglutide’s not for you. It can also affect blood sugar, so you might need to adjust insulin or sulfonylurea doses to dodge hypoglycemia. Your provider should check thyroid history, kidney function, and watch for pancreatitis before and during treatment.
Long-Term Considerations
Long-term safety depends on the drug’s mechanism. With ipamorelin, the worry is chronically high IGF-1 and what that might do to cell growth—human studies over years are limited. If you stay on it, regular labs and check-ins just make sense.
Semaglutide has longer-term data showing steady weight and glucose improvements, but you still need to watch for thyroid, gallbladder, and pancreatic trouble. Neither drug is recommended if you’re pregnant or breastfeeding.
Share your medical history, meds, and any cancer background with your provider before starting either. Ongoing follow-up and targeted bloodwork cut the risk of big side effects.
Dosage Guidelines and Administration
Ipamorelin calls for several small daily injections to trigger growth hormone pulses. Semaglutide is simpler—just a once-weekly shot at a set dose. Dosing, timing, and supervision all differ, and you’ll probably need tweaks for side effects, goals, or other drugs.
Ipamorelin Dosage Protocols
Most people use ipamorelin by subcutaneous injection two or three times daily to mimic natural GH rhythms. Typical single doses run 100–300 mcg, with total daily dose usually 200–600 mcg split up.
Inject near bedtime or before workouts to sync with nighttime GH release and recovery. Space injections by at least 4–6 hours for pulsatile secretion.
Cycles usually last 12–24 weeks if you’re chasing body-composition changes, since GH effects build slowly. Monitor IGF-1 and how you feel. If you get joint pain, fluid retention, or carpal tunnel symptoms, let your clinician know—sometimes a dose cut or break is needed.
Semaglutide Dosage Recommendations
For weight loss, semaglutide is a once-weekly subcutaneous shot with a slow ramp-up. Most start at 0.25 mg weekly for 4 weeks, then 0.5 mg for another 4 weeks, bumping up (maybe to 1.0 mg, 1.7 mg, and up to 2.4 mg) as tolerated and guided by your prescriber.
If you get nausea or GI upset, your provider might slow things down. Stick with the effective dose to keep weight off—stopping usually means weight comes back.
Kidney or liver disease? You might need dose tweaks or closer checks. If vomiting won’t quit, or you have severe belly pain or pancreatitis signs, call your provider right away.
Route of Administration Differences
Both drugs go under the skin, but how often and what device you use changes the experience. Ipamorelin means daily pens or vials with insulin syringes—so, multiple shots each day. Rotate sites and keep things clean.
Semaglutide comes in prefilled pens for once-weekly use, which is honestly a relief for most people. Early on, injection site reactions and mild nausea are common with semaglutide. Ipamorelin mostly causes local soreness or fluid shifts.
Protocols aren’t all the same, so get hands-on training from a clinician or nurse for mixing (if needed) and for injection technique. Keep both meds in the fridge as directed and jot down your doses somewhere.
Ideal Candidates for Each Compound
Ipamorelin fits people looking to boost growth hormone for better body composition, while semaglutide is more for folks who need serious appetite control and blood sugar help for weight loss.
Who Should Consider Ipamorelin?
Think about ipamorelin if you want to build lean mass, drop stubborn fat, or recover and sleep better because of low growth hormone. It works best for adults with age-related GH decline or those already lifting and eating enough protein.
If your blood sugar is normal but you want more muscle tone, easier joint recovery, or maybe better skin, talk to your clinician. Skip it if you have active cancer, pituitary disease that’s not managed, or if you’re pregnant.
Signs you might benefit: low energy, struggling to gain muscle despite training, or labs showing low IGF-1. Changes will be slow and depend a lot on your workouts, diet, and regular check-ins.
Who Benefits Most from Semaglutide?
Semaglutide makes sense if you need strong appetite suppression and real weight loss—especially with overweight, obesity, or type 2 diabetes. It cuts hunger and drops fasting glucose and A1C, so it’s handy when metabolic health is the focus.
It’s good for people who can’t control portions, snack too much, or have high blood sugar even after lifestyle changes. If you’re planning pregnancy or have a personal/family history of medullary thyroid carcinoma or MEN2, skip it.
You’ll probably see weight loss in weeks to months. Expect regular medical follow-up for dose tweaks and to manage side effects like nausea.
Cost and Accessibility
Price, insurance coverage, and how you get each drug are pretty different. Semaglutide is FDA-approved for weight loss and often covered; ipamorelin is usually compounded and paid out of pocket.
Pricing Comparison
Semaglutide’s brand-name versions (like Wegovy or Ozempic) often cost more per month, but insurance sometimes helps if you use it for diabetes or obesity. Without insurance, you might pay anywhere from several hundred to over a thousand dollars monthly, depending on dose and pharmacy. Generics or savings programs can lower the hit to your wallet.
Ipamorelin usually costs less per vial than semaglutide, but insurance rarely covers it. Most people pay cash at peptide clinics or compounding pharmacies. Monthly costs swing a lot based on provider, formula, and dosing, so compare per-dose and monthly prices before you buy.
Availability and Prescription Requirements
Semaglutide is FDA-approved for type 2 diabetes and long-term weight management at specific doses. You’ll need a prescription and follow-up visits for dosing and monitoring. Pharmacies and telemedicine services can fill it, so access is pretty broad if you’ve got a prescriber.
Ipamorelin is mostly available through specialty clinics or compounding pharmacies. Prescribers might offer it off-label for body composition or anti-aging, but insurance doesn’t usually help. Most clinics require an initial consult, baseline labs, and regular follow-up—so access depends on your area and the clinic’s setup.
User Experiences and Testimonials
People notice different changes in appetite, fat, and muscle tone depending on what they’re taking. Side effects and how fast results show up vary a lot, so it’s worth reading what users say about dosing, tolerability, and timelines.
Ipamorelin User Insights
Most users describe gradual changes with ipamorelin. Improved sleep, a bit more muscle tone, and steadier energy are common themes over weeks. Fat loss is slow and steady if you’re working out.
Side effects people mention include mild water retention, the occasional headache, and soreness at the injection site. Some who check labs see small bumps in IGF-1 and growth hormone, especially overnight. Sticking to workouts and protein seems key for body-composition changes.
Dosing routines differ, but many prefer a bedtime injection to boost nighttime GH. A few users warn that if you quit therapy but slack on lifestyle, results fade out fast.
Semaglutide Patient Stories
Lots of patients mention rapid appetite suppression and noticeable weight loss in a few months. Losing several percent of body weight in 12–24 weeks isn’t rare if you stick to dosing and diet.
Nausea, constipation, and a bit of fatigue are the usual complaints. Many suggest starting low and ramping up slowly to dodge GI issues. Some say their clothes fit differently before the scale really moves—maybe early fat loss at work.
People with diabetes or insulin resistance often see better blood sugar control. Plenty of stories mention cravings and portion sizes dropping fast, which seems to drive most of the weight loss.
Conclusion
You might lean toward Ipamorelin if you’re after better body composition, more lean mass, and speedier recovery. It works by boosting growth hormone release, supporting muscle and shifting fat a bit. Fat loss is usually mild if you use it alone.
Semaglutide is the pick if you need larger, clinically proven weight loss and appetite control. It drops hunger and improves blood sugar, so you’ll probably see bigger changes in body weight and fat. GLP-1 therapy tends to give more predictable results for weight loss.
Some people try combining approaches, but always check with a clinician first. Medical conditions, drug interactions, and your goals all change the risk and benefit. Your provider can fine-tune dosing, watch for side effects, and track your progress.
Key points at a glance:
- Ipamorelin: boosts growth hormone, better for lean mass and recovery.
- Semaglutide: suppresses appetite, drives bigger weight loss.
- Safety: both need medical supervision and individualized plans.
Let your health goals and medical history steer your choice. Regular check-ins and lifestyle stuff like diet and exercise matter most for long-term change.
Frequently Asked Questions
Ipamorelin mainly lifts growth hormone to change body composition. Semaglutide lowers appetite and helps blood sugar to cut calories. Each one has different timing, muscle effects, and safety trade-offs that’ll affect which fits your goals.
How do ipamorelin and semaglutide differ in how they promote fat loss?
Ipamorelin signals your pituitary to release growth hormone, which can break down fat and nudge calories toward lean tissue over time.
Semaglutide switches on GLP‑1 receptors so you feel less hungry and your stomach empties more slowly. You eat less, and that’s where the weight loss comes from.
Which option is more likely to preserve or increase lean muscle mass during weight loss?
Ipamorelin tends to favor lean mass by boosting growth hormone and IGF‑1 signaling. If you combine it with resistance training and a solid protein intake, you’ll probably keep or even gain muscle.
Semaglutide mostly works by reducing calorie intake, so most of the weight you lose comes from fat. It won’t directly raise growth hormone, but pairing it with strength training and enough protein can help protect your muscle.
How do expected changes in body composition compare between a peptide therapy and a GLP-1 medication?
With ipamorelin, you’ll likely see less total weight loss, but a bigger chunk of that loss comes from fat while your lean mass stays steady or goes up. Progress tends to be gradual and really depends on how you eat and move.
Semaglutide usually leads to bigger drops in weight and waist size, mostly from curbing appetite. Most of the weight lost is fat, though you could lose some lean mass if you’re not careful with strength work or protein.
What side effects and safety considerations most often influence the choice between these two treatments?
Ipamorelin side effects don’t usually get too intense—maybe some swelling where you inject, a bit of water retention, or mild joint aches. There’s not a ton of long-term safety data for healthy adults, so you’ll want a doctor to keep an eye on your growth hormone levels.
Semaglutide tends to cause nausea, diarrhea, or constipation for some folks, and occasionally gallbladder problems pop up. It’s backed by strong clinical trials for weight loss and diabetes, but it’s not a good fit if you’ve had certain thyroid tumors or pancreatitis.
How quickly do results typically appear for fat loss and waist reduction with each approach?
Ipamorelin changes show up slowly, usually taking a few months. You might spot better muscle tone or some fat loss after 8–12 weeks, but the bigger shifts come after three to six months.
Semaglutide tends to bring weight and waist drops within the first month or two as your appetite shrinks. Most studies report steady progress over several months, and bigger changes by the half-year mark.
Who is generally a better candidate for each option based on goals, and baseline body fat?
If you’re aiming to improve lean mass, body composition, or recovery—and you’re willing to exercise and keep tabs on your progress—ipamorelin might make sense. It’s probably a good fit for folks with modest fat loss goals or those interested in anti-aging and holding onto muscle.
On the other hand, semaglutide stands out if your main goal is losing a significant amount of weight or trimming your waistline, especially if you have obesity or type 2 diabetes. People who want faster, more dramatic weight loss and don’t mind the usual GLP‑1 side effects tend to do well with it.