Address
30 N Gould St.
Suite R, Sheridan, WY 82801, USA
TB-500 Dosage Guide: Evidence-Based Dosing, Safety Considerations, and Administration Tips
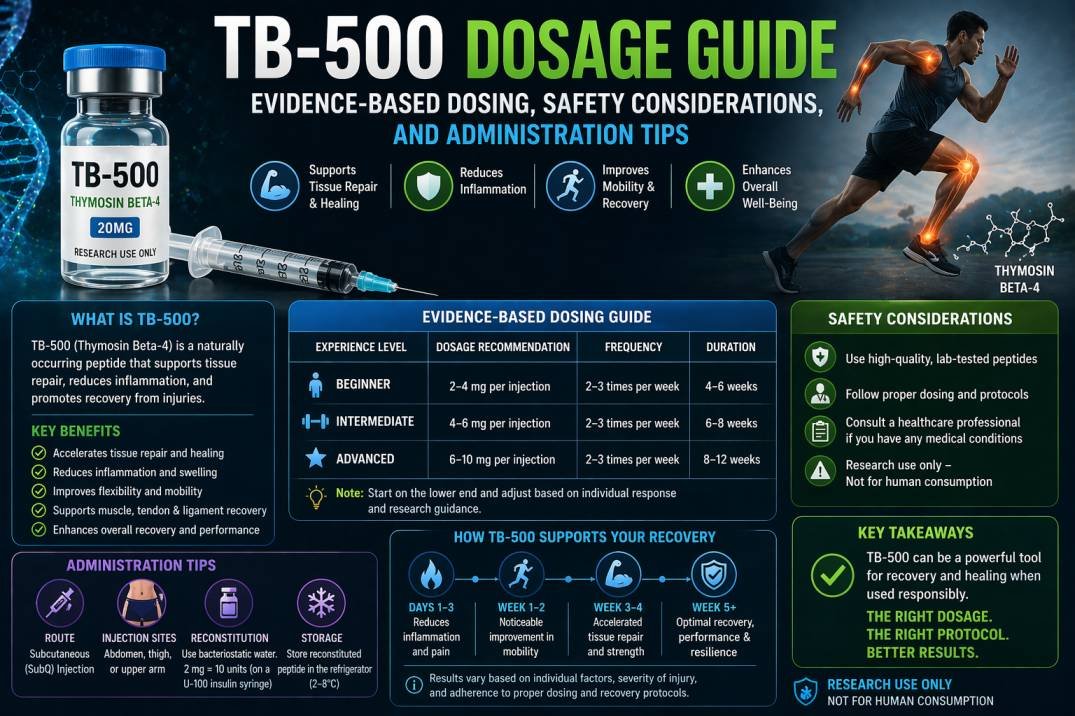
You want clear guidance on TB-500 dosing that helps you decide safe, practical steps without guesswork. For most people, a common approach uses a short loading phase followed by a lower maintenance dose, with exact amounts calculated from vial strength and body needs to balance effect and safety. This article breaks down the math, timing, and common protocols so you can plan dosing with confidence.
You will also get simple tips on mixing, injection technique, and what to watch for so you can lower risk and track results. Expect plain instructions and quick checks that help you avoid common errors and make sensible choices about cycles and sourcing.
Key Takeaways
- Start with a defined loading phase then move to a smaller maintenance dose.
- Calculate dose from vial concentration and your plan to ensure accuracy.
- Use correct mixing and injection methods and monitor for side effects.
Mechanism of Action: TB-500 Dosage Guide
TB-500 works by shifting cellular behavior to speed repair and reduce inflammation. It acts on the cytoskeleton, promotes cell migration, and influences blood-vessel formation in injured tissue.
Peptide Structure and Function
TB-500 is a short synthetic peptide that mimics a segment of thymosin beta‑4. Its sequence contains the active region responsible for binding actin, which helps control cell shape and movement.
When you use TB-500, the peptide increases the availability of actin monomers. That change lets cells extend filopodia and migrate into damaged areas faster. The peptide does not permanently alter your DNA; it modulates protein interactions in the cytoplasm.
TB‑500 is small and soluble, so it distributes systemically when injected subcutaneously or intramuscularly. That distribution supports healing at sites distant from the injection point.
Biological Pathways Involved
TB‑500 influences multiple pathways tied to wound healing. It upregulates genes and proteins involved in cell migration, such as actin-binding proteins, and can increase expression of VEGF, which promotes angiogenesis.
You will see reduced inflammatory signaling in some models, with lower levels of pro-inflammatory cytokines. TB‑500 also supports extracellular matrix remodeling by affecting metalloproteinase activity and collagen organization.
These combined effects—enhanced cell movement, new capillary growth, and controlled matrix remodeling—explain why TB‑500 can speed tissue closure and improve structural repair in animal studies and reported protocols.
Interaction With Other Compounds
TB‑500 is often discussed alongside peptides like BPC‑157 and growth factors. When combined, effects may be additive for tissue repair, but interactions depend on dose and timing.
You should avoid overlapping strong pro-angiogenic drugs without medical oversight, because multiple agents that increase VEGF or cell proliferation could raise risks in certain conditions. TB‑500 does not strongly bind to common prescription drugs, but immune-modulating or anticoagulant therapies could change outcomes.
Follow dosing guidance in the TB-500 Dosage Guide and discuss any stacking with a clinician. Keep track of timing, route (subcutaneous vs intramuscular), and total weekly dose to limit unexpected interactions.
TB-500 Dosage Guide: Standard Administration Protocols
This section gives clear steps for starting TB-500, how long to run it, and the dose split between initial and ongoing phases. Follow specific dosing, injection, and cycling guidance to reduce risk and track results.
First-Time User Recommendations
Start conservatively. Many users begin with 250–500 mcg twice weekly for the first 2–4 weeks to assess tolerance. Use an insulin syringe for accurate dosing and inject subcutaneously into fatty tissue, rotating sites each dose.
Keep a log of dose, date, injection site, and any side effects like mild soreness or fatigue. If you tolerate the initial period with no adverse effects, you can increase to common therapeutic levels such as 500 mcg twice weekly or a daily 500 mcg loading pattern, depending on your plan. Consult a clinician before changing dose if you have medical conditions or take other medications.
Typical Cycling Patterns
Common cycles balance on-phase treatment with recovery off-phase. A widely used pattern is 8 weeks on followed by 8 weeks off. Another option is 4–6 weeks on with 4–6 weeks off for shorter injuries or maintenance.
Track functional outcomes (pain, range of motion, strength) rather than only time. If improvement plateaus, pause the cycle and reassess after the off-phase. Always monitor labs and symptoms during longer cycles and halt use if you notice unexplained swelling, severe pain, or systemic signs.
Loading Versus Maintenance Phases
Loading builds tissue levels quickly; maintenance sustains effects. A typical loading protocol is 500 mcg daily for 1–4 weeks. This raises peptide exposure fast to kick-start repair signaling.
Maintenance doses drop to 250–500 mcg two to three times per week. Maintenance aims to keep benefits with fewer injections and lower overall exposure. Adjust maintenance based on response: extend, reduce frequency, or stop after functional goals are met.
Calculating Individual Dosages
You will calculate dose based on your weight, experience with peptides, and how often you want to split injections. Use precise math for milligrams (mg) and milliliters (mL) when you reconstitute vials, and track totals per week.
Dosage Ranges by Body Weight
Dose ranges often scale with body weight. A common approach uses a loading dose of about 0.02–0.04 mg per kilogram per day for the first 1–2 weeks, then a maintenance dose around 0.01–0.02 mg/kg every few days. For example, if you weigh 70 kg, a 0.03 mg/kg loading dose equals 2.1 mg per day (70 × 0.03 = 2.1 mg).
Convert mg to injection volume after reconstitution. If you add 2 mL bacteriostatic water to a 5 mg vial, concentration = 2.5 mg/mL. To inject 2.1 mg, draw 0.84 mL (2.1 ÷ 2.5 = 0.84 mL). Record calculations so you don’t misdose.
Adjust numbers to fit vial sizes (2 mg, 5 mg, 10 mg). Round volumes to match syringe graduations, and avoid doses that require impractically small or large volumes.
Adjusting Dosage for Experience Level
If you are new to peptides, start at the lower end of ranges. Begin with a conservative loading dose (for many, 0.02 mg/kg) and monitor response for 1–2 weeks before increasing. This reduces the chance of side effects and helps you learn proper injection technique.
If you have prior peptide experience and have tolerated TB-500 before, you may use the mid-to-upper range (up to 0.04 mg/kg) for loading. Experienced users often shorten loading to 1 week and move to maintenance sooner. Keep a log of dose, timing, and any effects so you can adjust safely.
Always adjust for health conditions and medications. If you have doubts, consult a qualified clinician; do not self-prescribe complex changes.
Splitting Daily and Weekly Amounts
Decide whether you want daily injections during loading or to split the weekly total into fewer injections. Daily loading often gives steady levels; for example, a 14.7 mg weekly target (70 kg × 0.03 mg/kg × 7 days) equals 2.1 mg daily. Alternatively, you can split the weekly total into three injections of 4.9 mg each on spaced days.
For maintenance, many people use 0.01–0.02 mg/kg total per week. You might inject once or twice weekly. Example: a 70 kg person at 0.015 mg/kg/week needs 1.05 mg/week; that can be one 1.05 mg shot or two 0.525 mg shots.
When splitting doses, keep each injection volume practical for your syringe and consistent timing. Mark your calendar and measure volumes precisely after reconstitution.
Methods of Injection
You will learn which injection route fits your goals, how to reconstitute and store TB-500 safely, and the steps to inject with lower risk of irritation or infection.
Subcutaneous vs. Intramuscular
Subcutaneous (SC) injections place TB-500 under the skin into fatty tissue. You use a short insulin needle (28–31 gauge) and inject at a 45–90° angle. SC is the most common for TB-500 because the peptide acts systemically and SC causes less pain and fewer bleeding issues.
Intramuscular (IM) injections put the dose deep into muscle. IM can absorb faster, but it raises the risk of soreness, bleeding, and hitting a nerve or blood vessel. Use a longer needle (22–25 gauge) for IM and pick the thigh, glute, or deltoid with proper technique.
Choose SC for routine maintenance and most injury protocols. Consider IM only if directed by a clinician for specific clinical reasons.
Reconstitution and Storage Procedures
Use sterile bacteriostatic water to reconstitute TB-500. Clean the vial top with alcohol. Draw the chosen volume of water into a syringe and inject it slowly down the vial wall to avoid foaming.
Typical reconstitution volumes range from 1 mL to 2 mL per 5–10 mg vial depending on target concentration. Note the concentration on your dosing chart so you can measure doses in units on an insulin syringe accurately.
Store reconstituted peptide in the refrigerator at 2–8°C. Keep it away from light and do not freeze. Unopened lyophilized vials stay cool and dry; follow manufacturer guidance for shelf life after reconstitution—commonly 2–6 weeks. Discard if you see cloudiness, particles, or a change in color.
Injection Best Practices
Always wash hands and clean the injection site with an alcohol swab. Rotate injection sites: use lower abdomen, outer thigh, or upper arm and avoid the same spot twice in a row. Rotate to reduce local irritation and scar tissue.
Use a new sterile needle and syringe for each injection. Remove air bubbles from the syringe and inject slowly. After injecting, apply gentle pressure with a clean swab for 10–20 seconds; do not rub the site vigorously.
Watch for signs of infection: growing redness, warmth, swelling, drainage, or fever. If you get persistent pain, large bruises, or odd symptoms, stop injections and consult a healthcare professional. Keep a log of dates, dose, site, and any reactions to track patterns.
Optimizing Results
Focus on dose timing, compatible peptide combinations, and daily habits that support tissue repair and reduce side effects. Small adjustments in when you inject, what you combine, and how you sleep and eat can change recovery speed and comfort.
Timing and Scheduling
Give TB-500 steady exposure during the first 2–4 weeks to kickstart repair. Many people use a loading phase of 2–5 mg split into 2–3 injections over the first week, then drop to 1–2 mg twice weekly for maintenance. Inject on consistent days—choose mornings or evenings—and stick to that routine.
Space injections at least 48–72 hours apart in maintenance. If you take once-daily low doses, inject at the same time each day to keep levels stable. Record dates, doses, and any reactions to track what works best for you.
Stacking With Other Peptides
Pair TB-500 with BPC-157 for complementary tissue healing; TB-500 supports cell migration and angiogenesis while BPC-157 targets gut and tendon repair. Common stacks: TB-500 (maintenance) + BPC-157 daily for 2–6 weeks when treating acute injuries.
Avoid stacking multiple immune-modulating peptides at once without medical oversight. Start one peptide first, monitor effects for 1–2 weeks, then add another. Keep doses conservative when you combine agents and note interactions like increased repair response or unexpected soreness.
Lifestyle Factors That Enhance Effectiveness
Prioritize sleep: aim for 7–9 hours nightly to support collagen synthesis and cell repair. Poor sleep reduces peptide benefits and slows recovery.
Eat protein-rich meals and include vitamin C and zinc to aid collagen formation. Stay hydrated; water helps nutrient transport to healing tissues. Limit alcohol and smoking, as both blunt repair mechanisms.
Use gentle progressive loading in rehab. Start light with mobility and strength work after pain eases. Controlled movement plus TB-500 often speeds functional recovery more than rest alone.
Side Effects and Safety Considerations
TB-500 can cause mild local reactions and has limited human safety data. You should weigh known injection risks, potential systemic effects, and gaps in clinical evidence before use.
Risk Assessment for Users
You should check medical history for bleeding disorders, autoimmune conditions, cancer, or active infections. Peptides like TB-500 may affect wound healing and cell migration; this matters if you have a current tumor, recent surgery, or are on immunosuppressants.
Consider medication interactions. Anticoagulants and platelet-affecting drugs raise bleeding risk at injection sites. Steroids or biologic immune therapies could change how your body responds.
Age, pregnancy, and breastfeeding also matter. There is little reliable human data for pregnant or nursing people, so avoid use in those cases. If you are under 18 or over 65, consult a clinician familiar with peptides.
Monitoring and Management
You should monitor injection sites and general health for the first weeks of use. Check sites daily for redness, swelling, warmth, or spreading bruising. Keep a log of dose, date, and any symptoms to detect patterns.
If you notice persistent redness or growing pain, stop injections and seek medical advice. For mild reactions, apply cold packs, clean the area, and avoid reusing needles. Use single-use sterile syringes and follow reconstitution hygiene to lower infection risk.
Have a plan for emergency symptoms. Know where to get urgent care if you develop high fever, severe shortness of breath, rapid heart rate, or signs of severe allergic reaction.
Signs of Adverse Reactions
Watch for local signs: increasing pain, expanding bruise, pus, or fever near the injection site. These suggest infection or significant inflammation and need prompt review.
Track systemic signs: unexplained weight change, new or worsening joint pain, persistent fatigue, or cognitive changes. Such symptoms may indicate an unexpected systemic response.
Recognize allergic and severe reactions. Hives, facial swelling, throat tightness, sudden dizziness, or difficulty breathing require immediate emergency care. If you develop abnormal bleeding, prolonged bruising, or signs of clotting, stop use and contact your clinician right away.
Legal Status and Sourcing
TB-500 is not FDA-approved for human use and faces varied rules worldwide. You should expect legal limits, sports bans, and product-quality risks when buying or importing it.
Global Regulatory Overview
In the United States, TB-500 is not an FDA-approved drug and appears on lists that restrict compounding pharmacies from making it for humans. That means legitimate prescription access is effectively unavailable, and possession or sale for human use may carry legal risk.
Many countries place TB-500 in a gray area: some allow sale as a research chemical, others require prescription or ban it outright. Professional sports ban TB-500 under WADA rules, so you risk disqualification if you test positive. Rules change often, so check national drug agencies and customs rules before you import or travel with it.
Safe Purchase Guidelines
Only buy TB-500 from sources that provide a Certificate of Analysis (COA) showing purity and lot testing. Look for suppliers who publish third-party lab results that match the product label and show >95% purity, free from common contaminants.
Avoid products marketed for “human use” by vendors in jurisdictions where TB-500 isn’t approved. If you consider research-grade material, treat it as a research chemical: use appropriate lab handling, keep documentation, and do not self-administer. When in doubt, consult a licensed medical professional or legal advisor about local laws and health risks before purchasing.
Tips for Long-Term Success
Keep a treatment log. Track doses, dates, injection sites, and any side effects. This helps you spot patterns and talk clearly with a healthcare provider.
Follow storage and handling rules. Store reconstituted peptide refrigerated and use within the manufacturer’s recommended window. Proper storage preserves potency.
Use consistent injection technique. Rotate sites and use clean supplies each time. This lowers infection risk and improves absorption.
Monitor your response and adjust slowly. Small changes to dose or frequency help identify what works without sudden shifts. Consult a qualified clinician before changing your plan.
Prioritize recovery habits. Good sleep, balanced nutrition, and controlled activity support tissue repair. These habits boost the effects of any peptide protocol.
Plan regular check-ins. Schedule lab tests or clinical reviews as advised to watch for adverse effects. Early detection keeps you safer over time.
Manage expectations. Benefits may be gradual and vary by person. Avoid high, frequent dosing to chase faster results; that raises risk.
Keep safety supplies and instructions handy. Have sharps disposal, antiseptic wipes, and emergency contact info near your kit. Being prepared reduces harm and stress.
Frequently Asked Questions
This section gives specific numbers and schedules you can use to plan TB-500 dosing, splitting vials, and combining TB-500 with BPC-157. It lists common loading and maintenance amounts, per-day calculations by weight, and examples for dividing a 10 mg vial across a typical cycle.
How do you calculate an appropriate daily amount based on body weight and goals?
Calculate weekly dose first, then divide by seven for a daily average. For example, a common loading weekly range is 4–6 mg; that equals about 0.57–0.86 mg per day.
If you prefer weight-based math, use about 0.03–0.06 mg per kg per week for many recovery protocols. For a 75 kg person that equals 2.25–4.5 mg per week, or roughly 0.32–0.64 mg per day.
Adjust toward the higher end for faster tissue repair goals and the lower end for maintenance or lower-risk use. Always document effects and adjust slowly.
What dosing schedule and frequency are commonly used during a loading phase versus a maintenance phase?
A common loading schedule: 2 mg twice weekly up to 2–3 mg twice weekly, totaling 4–6 mg per week. People often split these into two injections spaced 2–4 days apart.
Maintenance often drops to about 2.5 mg once weekly or 2 mg once weekly. Some users choose 2–2.5 mg every 5–7 days to keep levels steady.
What is a typical protocol when stacking with BPC-157 for soft-tissue injuries?
Common stacks use TB-500 for systemic effects and BPC-157 locally. Example: TB-500 loading 4–6 mg per week with BPC-157 at 250–500 mcg twice daily injected near the injury.
After 2–4 weeks, taper TB-500 to a 2.5 mg weekly maintenance while continuing BPC-157 for another 2–4 weeks, then reassess healing. Space injections to avoid injecting both drugs into the exact same site at the same time.
How do dosing ranges differ for bodybuilding-focused use compared with injury recovery use?
Injury recovery tends to favor higher short-term loading: 4–6 mg per week for 2–4 weeks, then maintenance at ~2.5 mg weekly. This aims at faster tissue repair.
Bodybuilding or performance use often uses lower maintenance dosing: 1.5–3 mg weekly with longer cycles. Users pursuing performance sometimes extend lower-dose maintenance for several months rather than repeated high-load cycles.
How should a 10 mg vial be divided across injections for a standard cycle length?
For a 4-week loading cycle at 5 mg/week, total need = 20 mg, so one 10 mg vial won’t cover it alone. For a single 6-week plan with 2-week loading at 5 mg/week then 4 weeks maintenance at 2.5 mg/week, total = 20 mg.
If you plan a 4-week cycle that uses 10 mg total, divide the vial into daily or per-injection aliquots. For example, if you inject twice weekly at 2.5 mg per injection, a 10 mg vial gives four injections (2.5 mg each). Use sterile technique and store aliquots per product guidance.
What is a common per-day amount when using a premixed BPC-157 + TB-500 blend?
Premixed blends vary, but a common formulation pairs TB-500 at 2–2.5 mg per week with BPC-157 at 250–500 mcg daily. That equates to about 0.29–0.36 mg TB-500 per day on average and 250–500 mcg BPC-157 per day.
If the blend is labeled by total mg per vial, calculate weekly needs and divide by administration days. For example, if the vial contains 5 mg TB-500 and 2.5 mg BPC-157 meant for two weeks, you would use ~0.36 mg TB-500 and ~0.18 mg BPC-157 per day.