Address
30 N Gould St.
Suite R, Sheridan, WY 82801, USA
TB-500 vs BPC-157: Comparative Benefits, Uses, and Safety Considerations
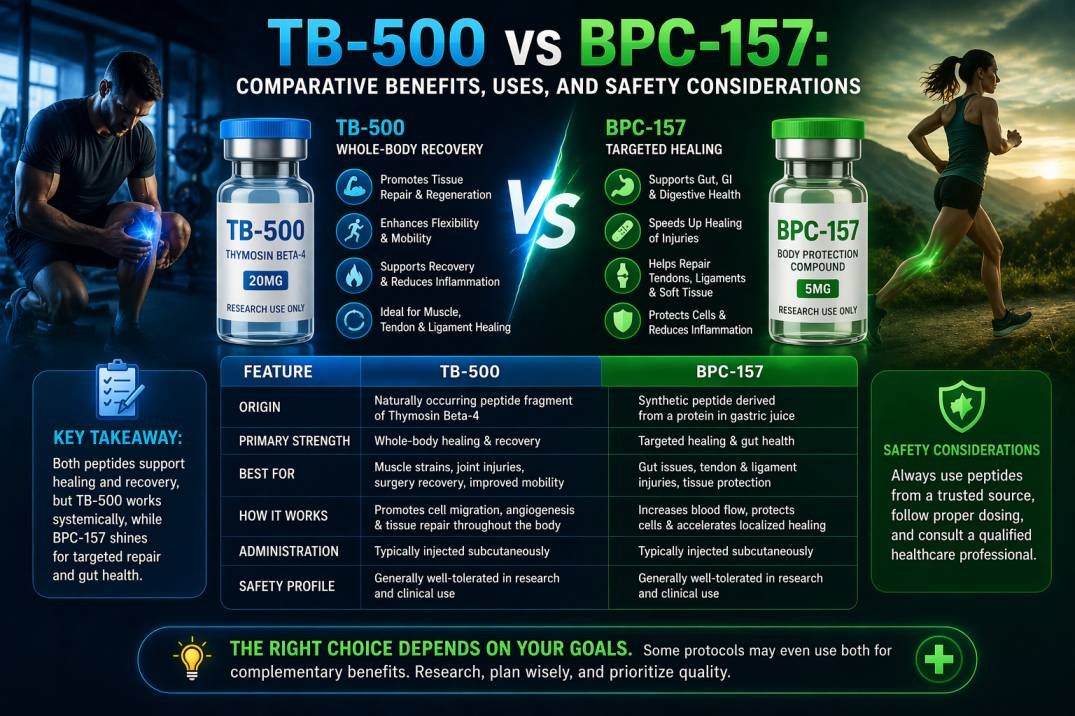
You’re after faster recovery and a clear answer. TB-500 generally helps with wide-area tissue repair and mobility, while BPC-157 seems to zero in on gut and tendon healing.
Pick TB-500 if you want broad tissue remodeling and flexibility. Go with BPC-157 for focused tendon, ligament, and gastrointestinal recovery.
This comparison digs into how each peptide works, where they really shine, and what risks or dosing quirks you should watch out for. You’ll get practical differences in mechanism, application, and results—no hype, just what actually matters.
Key Takeaways
- One peptide favors broad tissue repair and movement. The other targets tendons and gut healing.
- Each acts differently, so it’s worth matching the mechanism to your injury.
- Safety, dosing, and sourcing all affect which option makes sense for you.
Peptide Origins and History
Let’s look at where each peptide came from, what early research focused on, and how regulators treat them now. Here are the key dates, source molecules, and legal status highlights.
Discovery and Medical Background
BPC-157 is a 15–amino-acid fragment from a human gastric juice protein called Body Protection Compound (BPC). Researchers first pulled it from gastric tissue because it seemed to protect the gut and help wounds heal.
Early lab studies found BPC-157 modulates blood vessel signaling and inflammatory pathways. That led to experiments on gut ulcers, tendon healing, and organ protection.
TB-500 is a synthetic version of a component of thymosin beta‑4, a protein involved in cell migration and actin dynamics. Scientists created TB-500 to isolate the molecule’s regenerative part.
Initial lab work focused on wound repair, muscle and tendon recovery, and boosting cell migration after injury.
Initial Uses in Research
Early BPC-157 studies used rodent models for gastric ulcers, intestinal injury, and tendon tears. These experiments saw reduced inflammation and faster tissue closure.
Researchers also tested BPC-157 in nerve and liver injury models to see if it could protect more tissues, though always in preclinical settings.
TB-500 research started with wound-healing and cardiac injury models. Investigators studied how boosting cell movement affects scar formation and tissue remodeling.
Animal trials targeted tendon, muscle, and skin repair. Both peptides mostly stayed in preclinical studies, with just a few exploratory veterinary cases and not many controlled human trials.
Regulatory Status Overview
Neither BPC-157 nor TB-500 has FDA approval for human use. They’re usually sold as research chemicals labeled “for laboratory use only.”
That means suppliers and users handle them as unapproved compounds, with variable purity and dosing. Some sports and anti‑doping agencies ban these peptides or list them as reportable in competition.
Veterinary and experimental clinical uses happen in some places, but legal and quality standards vary a lot depending on where you are.
Mechanisms of Action
TB-500 and BPC-157 work on different molecules and pathways that control cell movement, blood vessel growth, and inflammation. One targets actin dynamics and broad tissue migration. The other tweaks growth factors and local angiogenesis.
Cellular Pathways Influenced
TB-500, a fragment of thymosin beta-4, mainly acts on the actin cytoskeleton. It boosts cell migration by increasing G-actin and improving filament turnover, helping cells move into injury sites and close wounds.
BPC-157, from gastric tissue, changes signaling tied to growth factors. It ramps up VEGF and can affect FGF and nitric oxide pathways, which encourages new blood vessel growth and protects cells from stress.
Both peptides reduce inflammation but by different routes. TB-500 shifts cell motility and repair machinery. BPC-157 changes local growth-factor signaling and vascular responses.
Differential Effects on Tissue Repair
TB-500 gives a systemic, pro-migratory effect. You’ll see faster cell recruitment and remodeling across tissues, which helps muscle, tendon, and skin repair.
Its action isn’t very tissue-specific, so it supports broad regenerative needs. BPC-157 delivers more localized, tissue-protective effects, with stronger impact on gut lining, ligaments, and connective tissue—places where growth-factor and vascular responses matter most.
It helps stabilize blood vessels and limits local tissue damage. Some people try combining the two, hoping to pair TB-500’s migration and remodeling with BPC-157’s angiogenesis and protection. Dosing, timing, and safety can get tricky, so weigh risks and evidence before mixing them.
Comparative Benefits for Injury Recovery
Both peptides help with repair but in different ways. One works locally on gut and tendons, while the other supports broader tissue remodeling and blood vessel growth.
Muscle and Tendon Healing
BPC-157 targets tendon and soft-tissue damage with focused, local effects. You might see quicker tendon bridging and less local inflammation when BPC-157 is used near the injury.
Studies and reports suggest it can protect tissue from further damage and help tendons reattach more cleanly. TB-500 works systemically to promote cell migration and actin remodeling, which helps muscle fibers realign and heal.
You could see improved muscle repair and less scar tissue over a wider area with TB-500. It also supports angiogenesis, so injured muscle gets better blood flow during recovery.
For targeted tendon repair, BPC-157 often stands out. For larger or multiple muscle injuries, TB-500’s systemic effects might help more.
Joint and Ligament Support
BPC-157 shows tissue-protective effects in ligaments and joint capsules, especially when you deliver it near the damaged site. You might notice less swelling and better ligament integrity as collagen organization improves.
TB-500 can reduce fibrosis and encourage new vessel growth around joints, which helps with nutrient delivery and the overall joint environment. That can speed recovery in complex joint injuries or when multiple tissues are involved.
If you’re aiming to reinforce a specific ligament or treat a local joint injury, BPC-157 may offer more focused help. If the joint injury involves broad inflammation, poor blood supply, or lots of scar tissue, TB-500’s systemic effects may be more useful.
Impact on Inflammation and Immune Modulation
Both peptides can reduce inflammation, but they use different pathways. One mainly changes cell movement and inflammation signaling, while the other boosts blood vessel growth and local tissue repair.
Anti-Inflammatory Properties
BPC-157 reduces local inflammation by improving blood flow and promoting tissue repair signals like VEGF. Animal studies show faster closure of small wounds and less swelling in injured tissue.
Its effects stay focused at the injury site, so inflammation elsewhere doesn’t change much. TB-500 lowers inflammation by promoting cell migration and actin remodeling, which helps immune and repair cells reach damaged areas and clean up debris.
Its action is more systemic, which can reduce broader inflammatory markers in preclinical models.
Immune System Effects
BPC-157 modulates immune behavior indirectly through better tissue integrity and local growth-factor signaling. Expect less immune activation at damaged sites, with fewer pro-inflammatory cytokines in animal studies.
It doesn’t act as a broad immune suppressant. TB-500 affects immune cell trafficking and wound-healing phases, changing macrophage and fibroblast activity to favor repair over prolonged inflammation.
This can tweak immune response timing but doesn’t seem to turn off immune defenses, at least in current preclinical data.
Potential Uses Beyond Injury Treatment
Both peptides seem to do more than just basic wound repair. You might see benefits for protecting tissues under stress or helping tissue regrowth in controlled settings, but human data is still pretty limited and safety questions are out there.
Tissue Protection Applications
You could use TB-500 or BPC-157 to protect organs or tissues under ongoing stress. BPC-157 has been studied for gut lining protection and lowering digestive tract inflammation.
TB-500 shows activity in promoting blood vessel growth and cell movement, which might help tissues survive low-oxygen or ischemic conditions. Researchers are looking at uses like protecting the stomach and intestines from NSAID damage, limiting muscle loss during inactivity, and preserving heart tissue after restricted blood flow.
Risks and dosing are unclear in humans, so these uses are experimental. Always weigh possible benefits against the unknowns.
Regenerative Medicine Possibilities
Think of these peptides as experimental tools in regenerative medicine research, not miracle cures. BPC-157’s effects on fibroblasts and collagen formation suggest roles in tendon and ligament repair models.
TB-500’s ability to modulate cell migration and angiogenesis makes it interesting for engineered tissue integration and better graft take. Researchers sometimes combine peptides with stem cells, scaffolds, or growth factors to speed integration and reduce scarring.
This could help surgical grafts or stubborn wounds heal in lab settings. But getting to routine clinical use will take controlled human trials to sort out efficacy, safety, and the best ways to use them.
Dosage Considerations and Administration Methods
Here’s what you need to know about dose ranges, typical schedules, and the main ways people use these peptides. Pay attention to dosing accuracy, cycle length, and delivery method pros and cons.
Standard Dosing Protocols
For TB-500, common research doses run from 2–5 mg per administration. Many start with 2 mg twice a week for 2–4 weeks, then taper to once weekly or a maintenance dose.
Cycle length is usually 4–6 weeks, but adjust based on how you respond. BPC-157 is usually dosed in micrograms—200–500 mcg per dose is standard.
A common approach is 200–300 mcg twice daily for 2–6 weeks, or once daily for maintenance. You can dose it locally (near an injury) or systemically.
Watch your total weekly exposure and adjust for body weight, injury severity, and changes in symptoms. Stick to the lowest effective dose and check in every 2–4 weeks. Don’t exceed recommended ranges without a pro’s input.
Forms of Delivery
Subcutaneous (under the skin) injections are the go-to route for both peptides. They’re simple enough for self-administration and give steady local or systemic absorption.
Many people inject BPC-157 near the injury to concentrate effects. Intramuscular injections work for deeper tissue delivery, especially for TB-500 if you want broad systemic effects.
IM dosing can give longer release but needs good technique to avoid irritation. Oral or topical BPC-157 exists, but absorption can be hit or miss.
Reconstituted powder in sterile water needs clean handling and refrigeration. Always use sterile technique, do your dosing math right, and follow the product’s instructions.
Safety Profile and Side Effects
Both peptides show low rates of acute reactions in animal studies and informal human reports, but risks depend on how you use them, the dose, and your health. Know the common short-term reactions and the lack of long-term data before you try them.
Short-Term Risks
You might get mild local reactions after injections—redness, swelling, or minor pain at the site. Usually, these clear up in a few days with basic care.
Some people report headaches, fatigue, or brief nausea. TB-500 has rare reports of allergic reactions, so watch for hives, trouble breathing, or rapid swelling and stop immediately if that happens.
Dose and frequency matter. Higher or more frequent dosing ups your risk of side effects.
If you take other meds or have an active infection, talk to a clinician. Interactions or masking of symptoms can happen.
Long-Term Considerations
Long-term safety data for both peptides are scarce. Most info comes from animal studies or small human reports, so there could be unknown risks with long-term use.
There’s some theoretical worry about effects on cell growth and blood vessel formation. If you have cancer, a history of tumors, or suspicious lesions, steer clear until an oncologist or specialist gives the okay.
Regular monitoring helps manage risk. Think about periodic blood tests, skin checks, and reporting new symptoms to your provider. Keep dosing records and stop if you notice unexpected weight changes, ongoing fatigue, or new lumps.
Availability and Purchasing Considerations
You’ll spot TB-500 and BPC-157 at plenty of online shops, research chemical outlets, and even a few clinics. Availability really depends on where you live, so it’s smart to check your country’s laws before you buy anything.
Quality swings a lot between suppliers. I’d suggest sticking with vendors who actually show you a batch-specific COA (certificate of analysis) and spell out their storage or shipping steps.
If a seller’s labeling is vague or they skip testing info, that’s a red flag. Sometimes you get what you pay for—cheaper peptides might skip third-party testing or get stored badly.
Peptides that come with refrigeration and proof of purity usually cost more, but you’re paying for peace of mind. Shipping and storage are a big deal for stability.
Many peptides need cold packs or even dry ice if they’re traveling far. Don’t hesitate to ask sellers about expiration dates, how they handle shipping, and what happens if your order arrives warm or damaged.
It’s worth thinking about legal and medical risks before you hit “buy.” Both of these peptides kind of float in a regulatory gray area in a lot of countries.
If you’re already on medication or have health conditions, talk to a real doctor before you get started.
Quick checklist:
- Check if it’s legal where you live or if clinics offer it.
- Ask for a COA and batch number every time.
- Double-check that shipping and storage instructions keep it cold.
- Compare prices, but weigh them against testing and safe handling.
- Have a chat with a healthcare provider about dosing and safety.
Current Research and Future Perspectives
Most of the research on TB-500 and BPC-157 comes from animal models, a few small human case reports, and some early safety data. There’s a lot of preclinical work ahead, and clinical trials seem to move slowly and carefully.
Key Clinical Studies
You’ll mostly see controlled data for these peptides in animal studies—stuff like tendon, ligament, and skin repair. Rodent experiments often report faster wound healing, less inflammation, and better collagen structure after dosing.
Human evidence is still thin on the ground. A few case reports and small open-label series describe less pain and better function after tendon injuries, but these aren’t randomized and don’t use standard dosing.
So far, safety signals in small groups look okay, with few acute problems, but we really don’t know much about long-term safety or the right dosing yet.
Regulatory-grade clinical trials are rare. If you’re thinking about clinical use, I’d say keep an eye out for randomized, placebo-controlled studies with solid endpoints—pain scores, imaging, biomechanical testing, all that.
Emerging Areas of Interest
There’s some buzz around combining the two peptides and figuring out if they work better together. Researchers are digging into how TB-500 might affect cell migration and actin, while BPC-157 gets attention for blood vessel growth and gut-to-muscle signaling.
Some new models stack both peptides to see if they help with chronic tendon problems or tricky wounds, measuring things like blood vessel density and collagen types. I’d keep an eye out for larger safety registries and better ways to check peptide purity.
Translational work is also poking at delivery methods—think slow-release formulas or local injections—to limit how much ends up in your system and better target injured tissue. This research could shape practical dosing and safety if these peptides ever go mainstream.
Final Words
Choosing between TB-500 and BPC-157 really depends on what you’re trying to heal. TB-500 works systemically and can help with tissue remodeling across broader areas.
BPC-157, on the other hand, tends to focus on localized gut and soft-tissue repair. That difference can matter a lot if you’re dealing with a nagging injury in one spot versus something more widespread.
Timing and dosing aren’t identical. TB-500 sticks around longer, while BPC-157 usually needs more frequent, targeted dosing to get results where you want them.
Honestly, safety and evidence should be at the top of your list. Most of what we know comes from preclinical studies, so there’s a fair bit of uncertainty for people. Chat with a qualified clinician before you try any peptide—seriously, don’t skip that step.
Quick comparison (high level):
- TB-500: systemic, supports actin dynamics and cell migration.
- BPC-157: local tissue protection, gut and tendon affinity.
Try to keep your expectations in check. Peptides aren’t magic bullets, and everyone responds differently. Make sure you prioritize safety, get your peptides from trusted sources, and talk things over with a professional.